


July 27, 2023
This paid piece is sponsored by Siouxland Oral & Maxillofacial Surgery.
If you’re missing a tooth and want to “fill that gap” to make things more esthetic or more functional, there are a few things to consider. This thought process can happen when you are making decisions at the time you lose your tooth and want a replacement, or when you have already lost your tooth a few years ago and now want a replacement.
In the first case, when you lose a tooth and want a replacement immediately or very soon, you have a few options. Permanent options include a traditional “bridge” that requires removing tooth structure from adjacent teeth to attach the prosthetic tooth, a Maryland bridge that bonds the tooth replacement to the teeth on either side, or a dental implant.

In the second case, you can choose to do nothing and have the space where your tooth used to be, or have a removable prosthesis such as a partial denture, a flipper or an Essix retainer. All of these have tooth replacement but are removable.
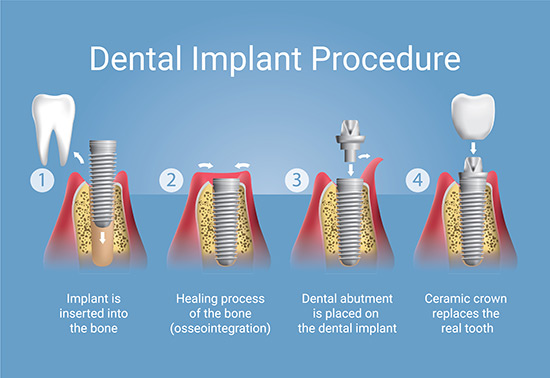
Both options have pros and cons. But for today’s discussion, we will focus on dental implants. For many patients undergoing tooth extraction, there is the possibility of immediate dental implant placement at the time of extraction. There is usually a requirement for bone grafting along with the placement of the dental implant. Documented failure rates for “immediate” are slightly higher than extracting the tooth, waiting for a period of six to nine months, and then placing the dental implant. The key determinant of when to place the implant is evidence on x-ray that the hard outer shell of the bone, called cortical bone, has re-formed.

One thing to understand is that dental implants are round in cross-section and tooth extraction sockets are elongated in cross-section. So when placing a dental implant in a new extraction socket, there will always be a gap between the round circular implant and the elongated extraction site. This gap must be filled with a bone graft material to act as a road map for the body to begin the process of building your own bone in that area. This newly formed bone will eventually meet and bond with the dental implant.
The main success factor for immediate dental implant placement is the preservation of bone all the way around the implant. Typically, it is the bone closest to the lips—the buccal bone—that is most at risk of fracture during tooth extraction, and this is the bone we want to preserve. One technique to preserve the buccal bone is the “shell or shield technique” where you intentionally leave a small shell of tooth structure attached to the buccal bone, along with cancellous bone grafting to preserve the area.
Another more successful technique is to remove the tooth, place the implant, and use a bone graft to fill the gap between the dental implant and the oral bone.
A third technique is to remove the tooth, perform a bone graft, wait six to nine months for the bone to heal, and place the dental implant later. This time gap may seem like a long time to wait, but you need to allow a period for the bone to heal. On x-rays, you’ll actually see this hard outer shell of bone forming in six to nine months. This hard outer surface is called the cortex. Once the crust forms, healing is complete.

Bone grafting at the time of extraction when no immediate implant is placed is known as ridge-preserving grafting. The purpose of the graft is to preserve bone volume in this area for future implant placement in six to nine months. Over time, bones that are not stimulated by tension atrophy. Your teeth are held to the bone by a ligament – like little rubber bands – so as forces are applied to the tooth, the tooth pulls on the ligament and the ligament pulls on the bone. This stimulates bone metabolism. Without this pulling effect, the bone atrophies. One way to compensate for this process is the ridge-preserving graft. If, however, you choose this graft and wait a few years for implant placement, then even the ridge-preserving graft atrophies. Therefore, if you receive this graft, it is important to place the implant between six to 12 months later.
In some cases, ridge-preserving grafting is unnecessary, such as in the maxilla where the maxillary sinus descends and thins the bone so much that you have to complete a bone graft in the sinus to place a dental implant. In this example, the body will itself fill the extraction site with bone. Later, you can do the sinus lift bone graft and most of the time even place the implant at the same time. The reason a ridge-preserving graft may be unnecessary in this case is because the ridge-preserving graft is designed to keep the bone in the buccal cortex and keep the bone vertical.
The implant should be placed 2 to 3 mm below where the teeth attach to the bone, and in six to nine months, bone atrophy will not occur so quickly in most people as to erode the bone in a vertical dimension. If the extraction of the tooth is completed correctly, you will not need a bone graft to stabilize the bone in a horizontal dimension in most cases.
The point here is that ridge-preserving grafts in the posterior maxilla in some cases are not necessary in preparation for dental implants. So if your provider says you need one, ask them to explain why.
To recap, be sure to preserve the oral bone, bone graft the gap, and you may or may not need the ridge-preserving graft if you are delaying dental implant placement.
These are advanced techniques that are not taught on the faculty in dental school. And it usually takes several supervised surgeries to learn how to do it right. If your provider wants to provide you with these services, ask them how many of them they completed under the direct supervision of their teachers at school or at the residence. The answer should give you confidence that your provider can manage the surgery, has alternative procedures you can rely on to complete the case, and can manage any complications that arise.
Before the dental implant, other procedures may be needed to prepare for success